Invisalign ClinCheck: 5 reasons to work with it
Introduction: Initial Considerations If you work with aligners, I'm sure that more than once you've considered changing brands, although most probably
Sequential distalisation of the lower arch with aligners is a relatively predictable and effective treatment for resolving sagittal discrepancy. Before opting for this solution to treat the Class III presented by the patient, we must determine the limits that exist for this movement.
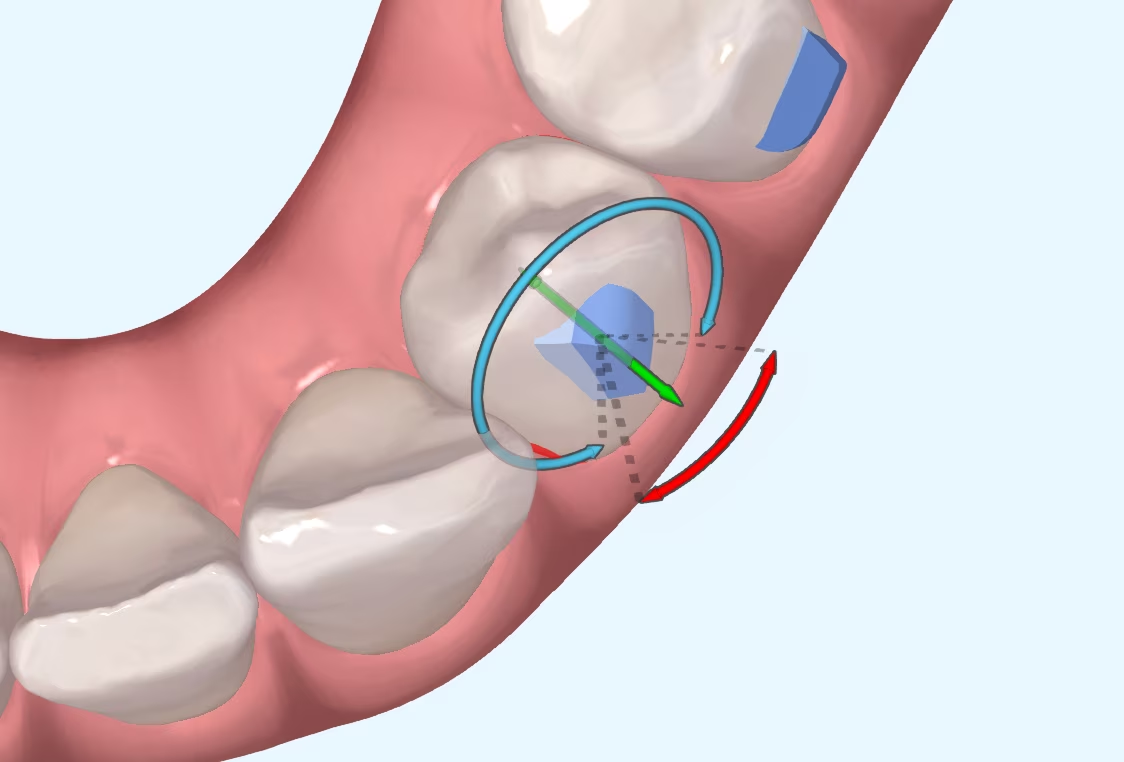
The limits of distalisation do not depend on the movement itself, although the more distalisation we desire, the more difficult it will be to achieve without auxiliary techniques and the worse the root control of the molars will be. This is a matter of course. The real limit is given by the patient's anatomy. The mandible is a structure with more limiting characteristics than the maxilla, making the movements of the teeth of the lower arch more complex.
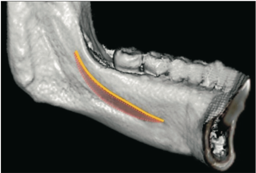
Classically, the method for deciding the amount of distalisation possible was to measure the distance between the mesial side of the mandibular ramus and the distal side of the crown of the second molar on the panoramic radiograph and the lateral teleradiograph. This information served as a "guide" or approximation to know how many millimetres we could distalise. However, it is highly inaccurate for two reasons:
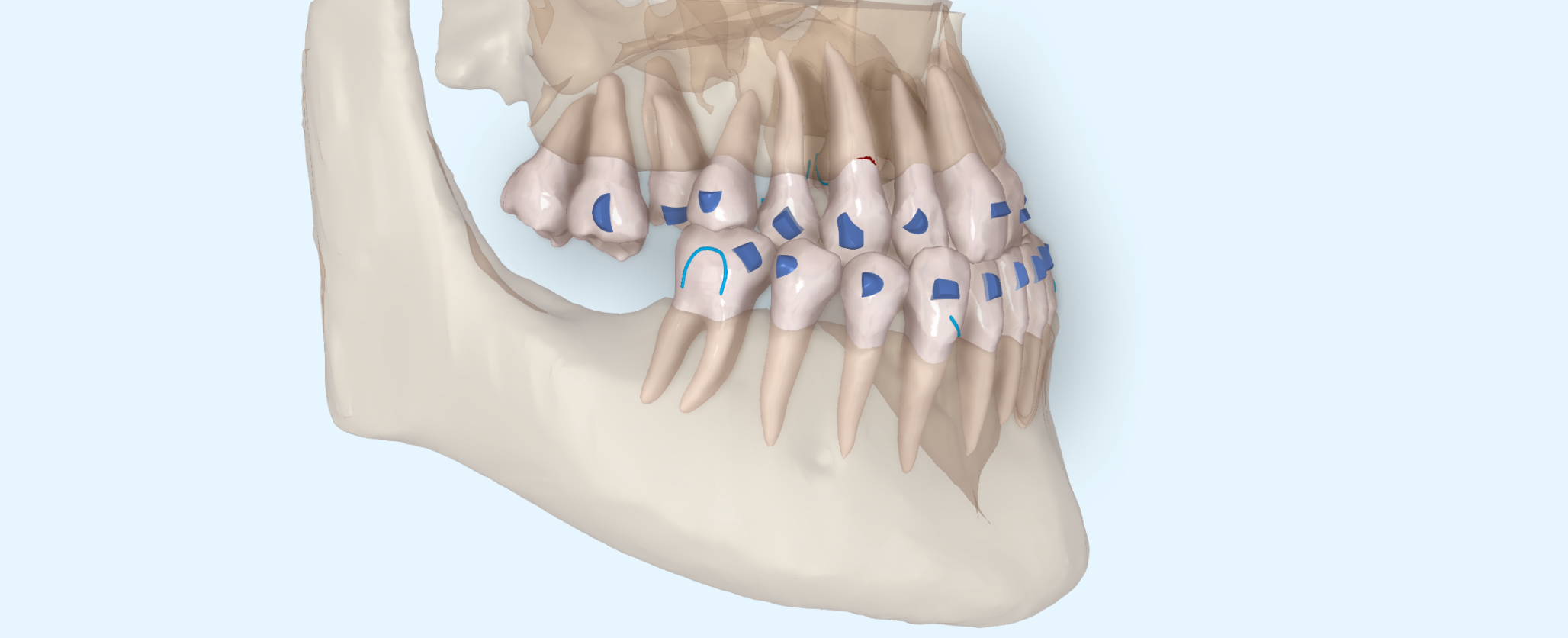
It is not compulsory to perform a CBCT on all our patients, but in some situations we can obtain very valuable data with which to optimise treatment. This is the case of Class III patients in which we want to distalise the lower molars. In a CBCT, unlike a panoramic X-ray, we can see what the mandibular body and ramus look like from all planes of space, measure the thickness of the corticals and determine the relationship between the roots of the molars and the retromolar bone. In other words, with CBCT we can better see the "path" that the molars have to follow when they are distalised and how far they can go in a relatively predictable way.
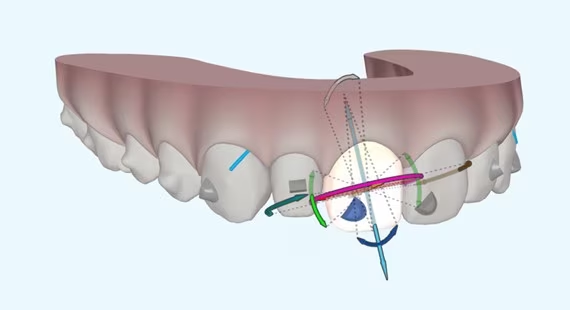
As the root surface of the second molar and the lingual cortex are not parallel, the distance between them will not be equal at all points of the root: as we move apically, the distance between the root and the cortex will be less. Paradoxically, if we had the ability to move the molars en masse, the amount of distalisation possible would be less than distalising them with some coronal tilt, which is the movement that actually occurs. Or, perhaps, this lack of control of mass movement can be aggravated when the apical part of the root contacts the lingual cortical bone and a fulcrum appears on which the tooth pivots if we continue to distalise it... who knows?
After this reflection, we pose the question: do you consider CBCT to be essential in these cases?
Kim S et al. Mandibular skeletal posterior anatomic limit for molar distalization in patients with Class III malocclusion with different vertical facial patterns. Korean J Orthod 2021;51(4):250-259
Introduction: Initial Considerations If you work with aligners, I'm sure that more than once you've considered changing brands, although most probably

Introduction I suppose many of you are familiar with the myth of Achilles, the Greek hero who was submerged as a child in the River Styx by his mother in order to

What is CBCT? CBCT is a medical imaging technique that uses a special type of computed tomography (CT) scan to obtain three-dimensional images.
Challenges of Overbite In the more than 20 years that we have been working with invisible orthodontics, we have gone from considering some malocclusions "impossible" to daring to

It is not a question to make us feel guilty. It is only a question that invites us to reflect, to think about the impact we can have in