Invisalign ClinCheck: 5 reasons to work with it
Introduction: Initial Considerations If you work with aligners, I'm sure that more than once you've considered changing brands, although most probably

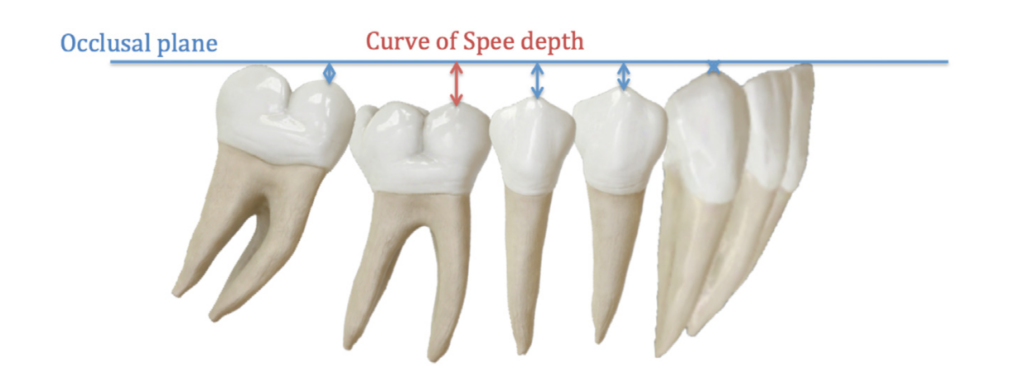
The curve of Spee is the natural curvature of the occlusal plane that follows the anatomical shape of the mandibular arch. An excessive Spee's curve can lead to various problems such as excessive wear of the anterior teeth, periodontal problems or joint disorders. This last aspect is frequently found in cases where the increased curve of Spee produces an anterior contact during closure that forces the patient to retroposition the mandible, impacting the condyle into the joint.
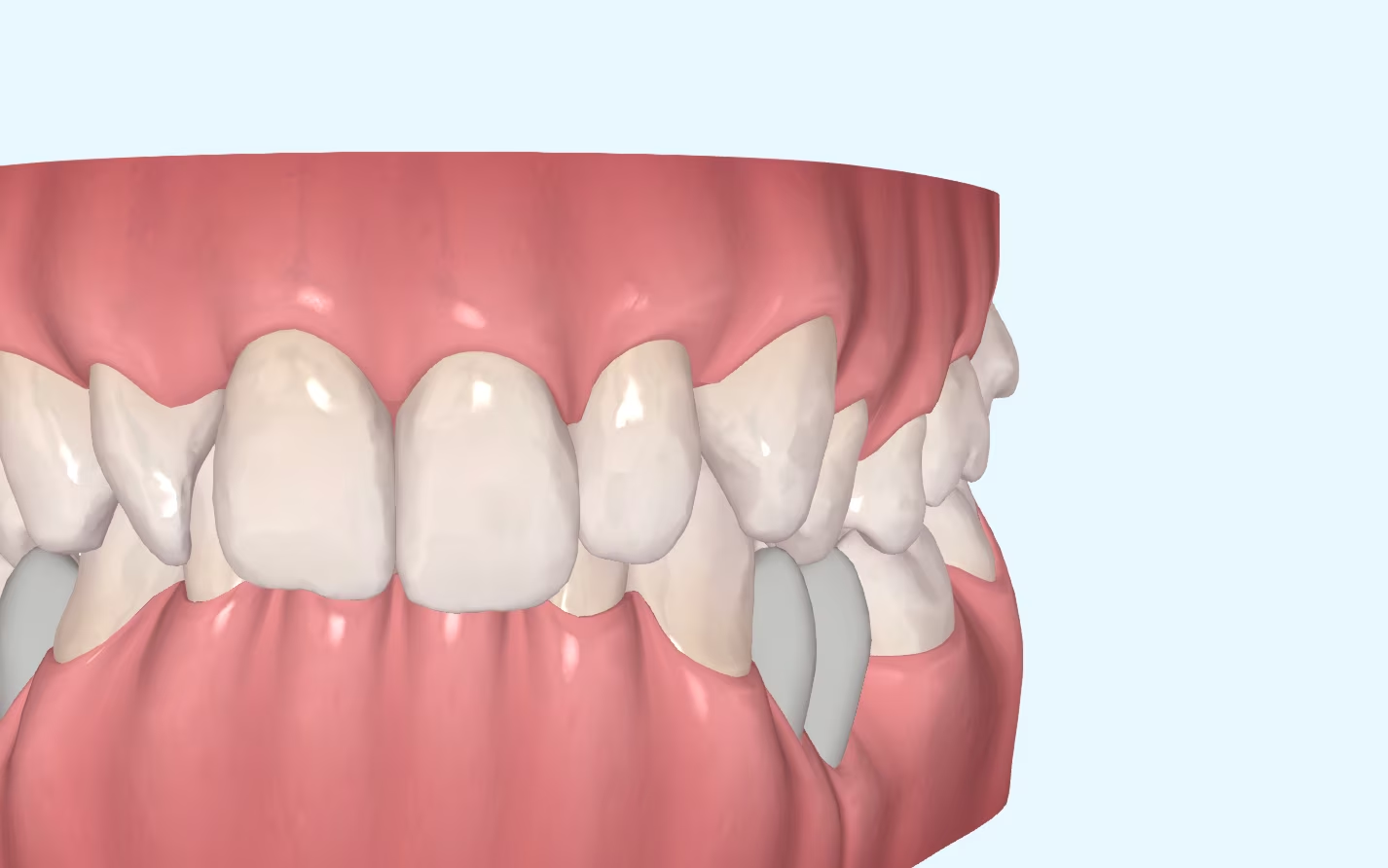
If we focus on the mechanics of orthodontic treatment, an increased curve of Spee can affect the correction of different problems. Although the curve of Spee is categorised as a vertical plane problem, it will also affect the sagittal problem if not fully corrected. This is often seen in Class II cases with an increased overbite. When we do not correct the overbite, i.e. when we do not level the lower curve of Spee, anterior contacts will appear that will block the mesialisation of the lower arch and will not allow the case to be completed in Class I.

If we look back to when we were working with brackets, when the curve of Spee was not corrected, the contacts between the brackets of the lower incisors and the palatal faces of the upper incisors also blocked this sagittal correction.
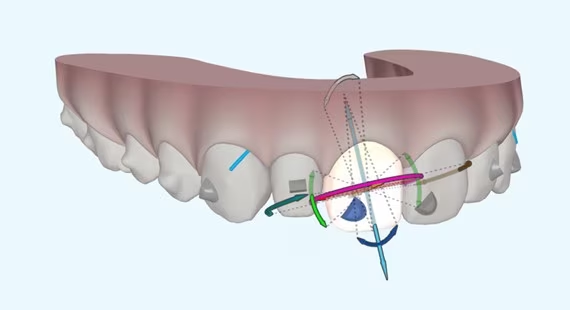
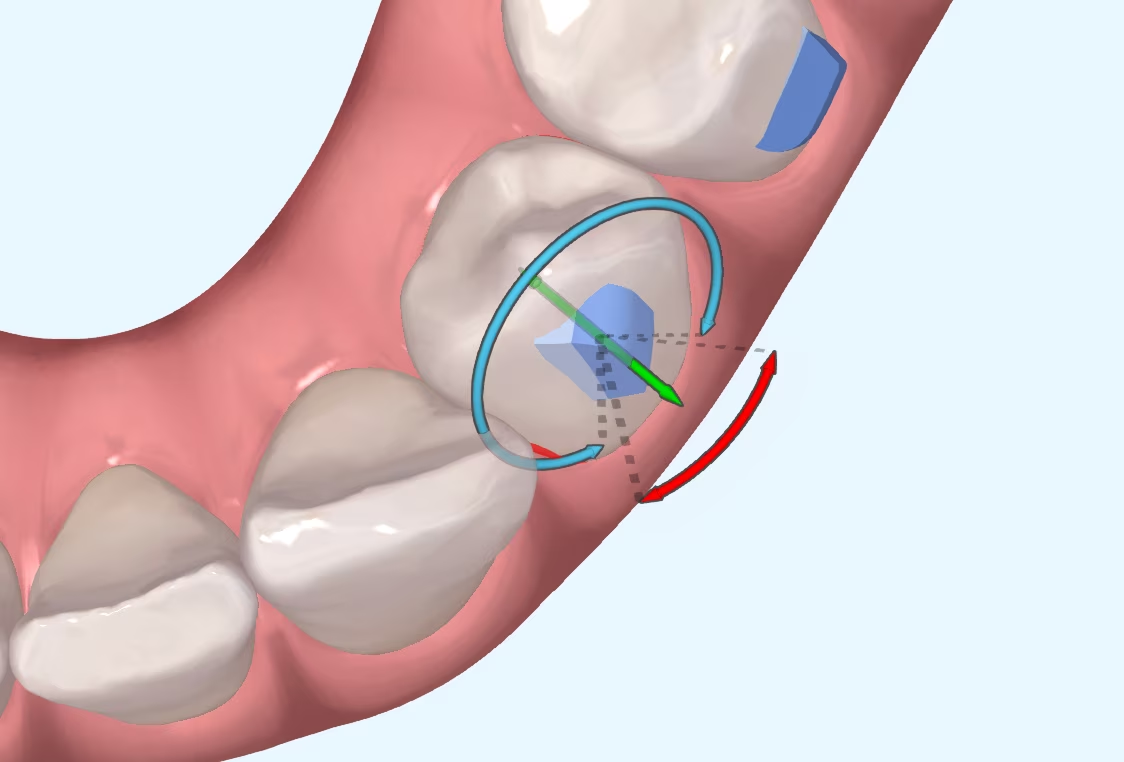
In orthodontics there is no appliance that has a predictability of 100%. For this reason, when we want to level the curve of Spee, we make overcorrections. In traditional orthodontics, as the archwires are not able to flatten the curve of Spee completely, archwires with a reverse curve shape were used or bends were made between premolars and canines, for example, to increase the intrusion force in the anterior region and level the lower arch adequately. When working with aligners, we will do something similar. We will apply a mechanic in the virtual planning that will allow us to counteract the inability of the aligner to achieve the movements at 100%. To do this, we will increase the intrusion of the anterior teeth and the extrusion of the posterior sectors, premolars and first molars. With this we will have a final position in the ClinCheck or in the Approver different to what we really want to achieve, but, just as the reverse curve arch is not our real final objective, what appears in a programme will not be either.
Fortunately, we are confident that these overcorrections, to a greater or lesser degree, work. Studies comparing the effectiveness of braces and Invisalign in intruding or levelling Spee's curve have found that both tools achieve relatively similar results. Knowing this, we can expect that, by applying the same strategy with aligners as we did with braces, we will obtain similar results.
And now we ask ourselves the question: how many millimetres of overcorrection do we do? There is no perfect answer. If we base it on the average predictability percentage of intrusion, we can make an estimated overcorrection of 40 or 50 % more than the necessary intrusion, but we cannot think that it is a perfect overcorrection either. The averages are made up of peaks and valleys, i.e., within that 40 % of predictability, there are patients where the predictability will have been, for example, 60 % and in other patients, 20%.
As we do not know the real predictability that the planned intrusion will have on each of our patients (there are many factors that affect it), it is advisable to always do more intrusion than necessary. Do not be afraid to exaggerate overcorrections, as you can stop at any time during the treatment. It is not necessary to reach the last aligner of the phase.
If, for example, we have a first phase of 40 aligners, but we observe that in stage 30 the curve of Spee is already level, we can stop the treatment there, avoiding giving the patient more aligners that could over-intrude the lower incisors and canines. Just as in some patients we will have the reverse curve arch active for more months than in others, we will try to do something similar with the aligners.
We are the ones who control the treatment.
Final advice: In orthodontic treatment, unless it is an open bite, it is advisable to finish with the curve of Spee flat. Over the years, the curve of Spee tends to increase, and in this way we will be able to prevent future problems and finish the cases in a more stable way.
Goh S et al. The predictability of the mandibular curve of Spee leveling with the Invisalign appliance. Am J Orthod Dentofacial Orthop 2022;162:193-200.
Rozzi M et al. Leveling the curve of Spee: Comparison between continuous archwire treatment and Invisalign system: A retrospective study. Am J Orthod Dentofacial Orthop 2022;162:645-55.
Introduction: Initial Considerations If you work with aligners, I'm sure that more than once you've considered changing brands, although most probably

Introduction I suppose many of you are familiar with the myth of Achilles, the Greek hero who was submerged as a child in the River Styx by his mother in order to

What is CBCT? CBCT is a medical imaging technique that uses a special type of computed tomography (CT) scan to obtain three-dimensional images.
Challenges of Overbite In the more than 20 years that we have been working with invisible orthodontics, we have gone from considering some malocclusions "impossible" to daring to

It is not a question to make us feel guilty. It is only a question that invites us to reflect, to think about the impact we can have in