Invisalign ClinCheck: 5 reasons to work with it
Introduction: Initial Considerations If you work with aligners, I'm sure that more than once you've considered changing brands, although most probably

We are all attracted to the concepts of "predictability" or "reliability". We want to offer the best guarantees to our patients in everything we do (and, incidentally, to sleep soundly), but, fortunately or unfortunately, biology is not as exact a science as mathematics.
As we have already discussed on other occasions, the development of aligners opened new doors for the correction of sagittal problems, one of them being the sequential distalisation.
Distalisation is not an easy movement to achieve. Traditionally, appliances such as pendulums or extraoral anchors were used to ensure that the forces applied were sufficiently effective to achieve distal movement of the molars, affecting the anterior teeth as little as possible. These appliances work very well, but they are uncomfortable and are not as easily affordable for today's patient profile. This is why the alternative of aligners is so attractive.
But before we start distalising, it is important to understand how the programmed movements are expressed or, in other words, what percentage of predictability our ClinChecks or Approvers will have.
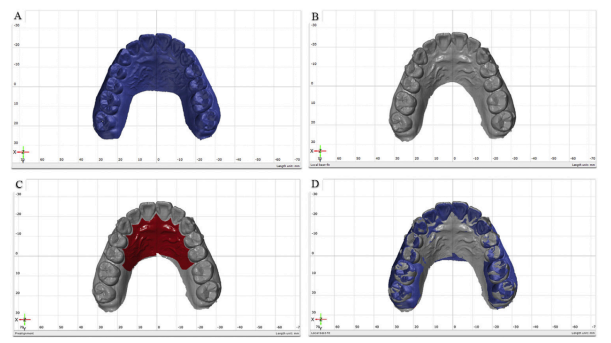
There are a multitude of studies that analyse the predictability but today we are going to review one published by Safi et al. in which they analyse, by superimposing digital models (using the palatal rugae as a reference), the difference between the planned results and those obtained in the patient after treatment with aligners.
The palatal ridge area is a relatively stable and reproducible structure on the dental model that can be used for registration and superimposition of serial jaw models in aligner treatments. This area is formed by the tissue "ridges" located in the anterior part of the hard palate, which are unique for each individual and can serve as reliable landmarks. This method of analysis allows the initial models to be reliably superimposed on the final phase models, allowing the amount of tooth movement during treatment to be accurately assessed.
The results of the study showed that the planned upper molar distalisation values on the Clincheck were significantly higher than the values achieved in the patient's mouth. The results are shown in the following table:

There are many factors that can contribute to these differences, such as improper sequencing, non-use of attachments or loss of anchorage that occurs in the anterior teeth when attempting to distalise the molars.
This study provides us with interesting information by using a very reliable measurement method. The findings suggest that the planned millimetres of molar distalisation in the Clincheck may overestimate the actual results. What do we learn from these results? That we should be aware of this when planning our aligner treatments.
Knowing these results, we have to optimising treatments to achieve the greatest possible predictability in these movements. Here are a few tips:
Saif BS et al. Efficiency evaluation of maxillary molar distalization using Invisalign based on palatal rugae registration. Am J Orthod Dentofacial Orthop 2022;161:e372-e379
Introduction: Initial Considerations If you work with aligners, I'm sure that more than once you've considered changing brands, although most probably

Introduction I suppose many of you are familiar with the myth of Achilles, the Greek hero who was submerged as a child in the River Styx by his mother in order to

What is CBCT? CBCT is a medical imaging technique that uses a special type of computed tomography (CT) scan to obtain three-dimensional images.
Challenges of Overbite In the more than 20 years that we have been working with invisible orthodontics, we have gone from considering some malocclusions "impossible" to daring to

It is not a question to make us feel guilty. It is only a question that invites us to reflect, to think about the impact we can have in