Invisalign ClinCheck: 5 reasons to work with it
Introduction: Initial Considerations If you work with aligners, I'm sure that more than once you've considered changing brands, although most probably
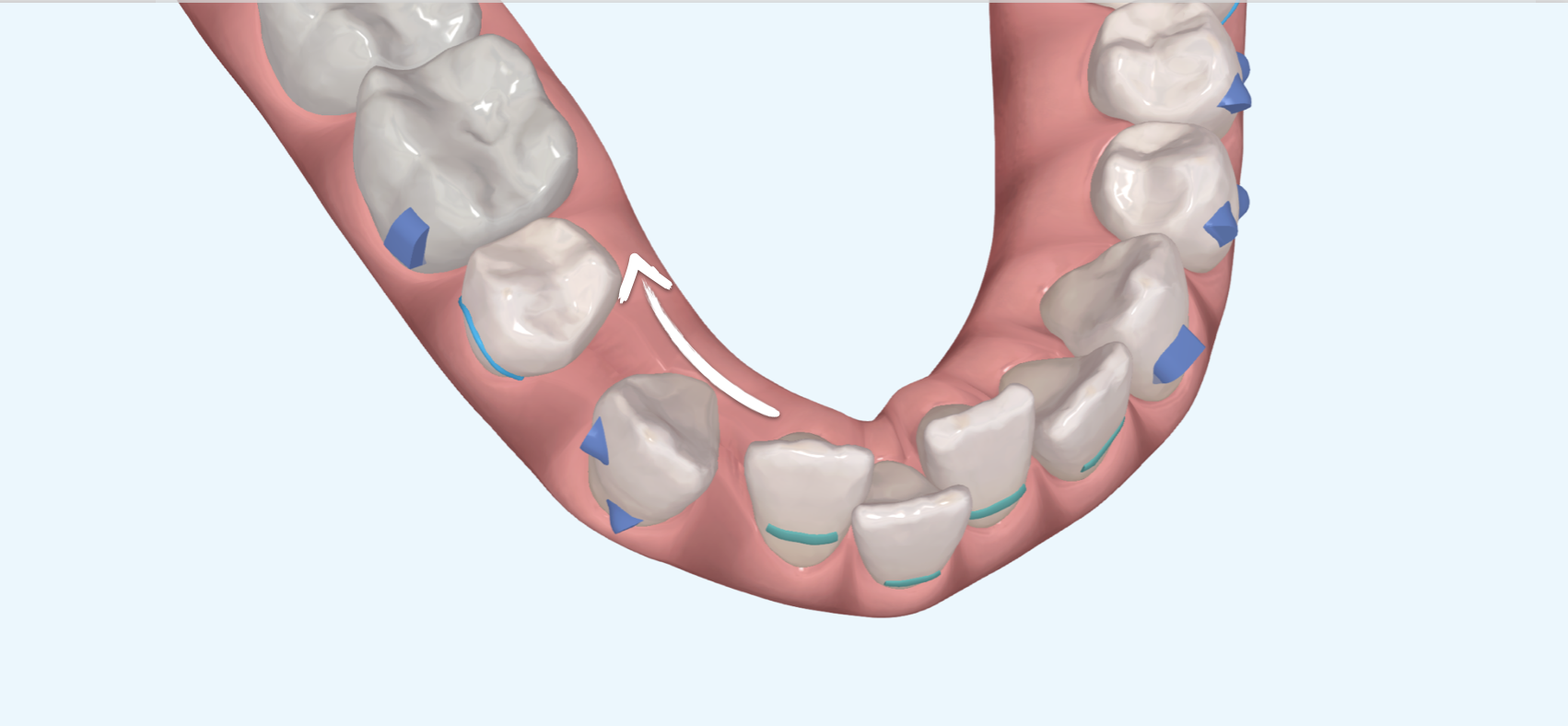
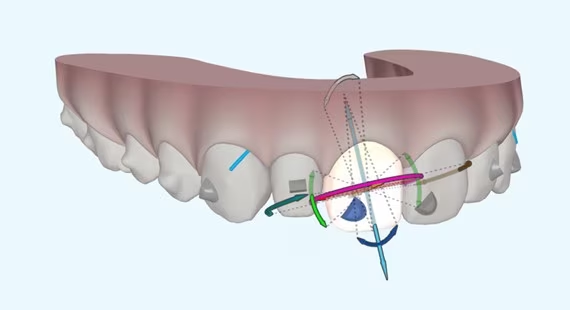
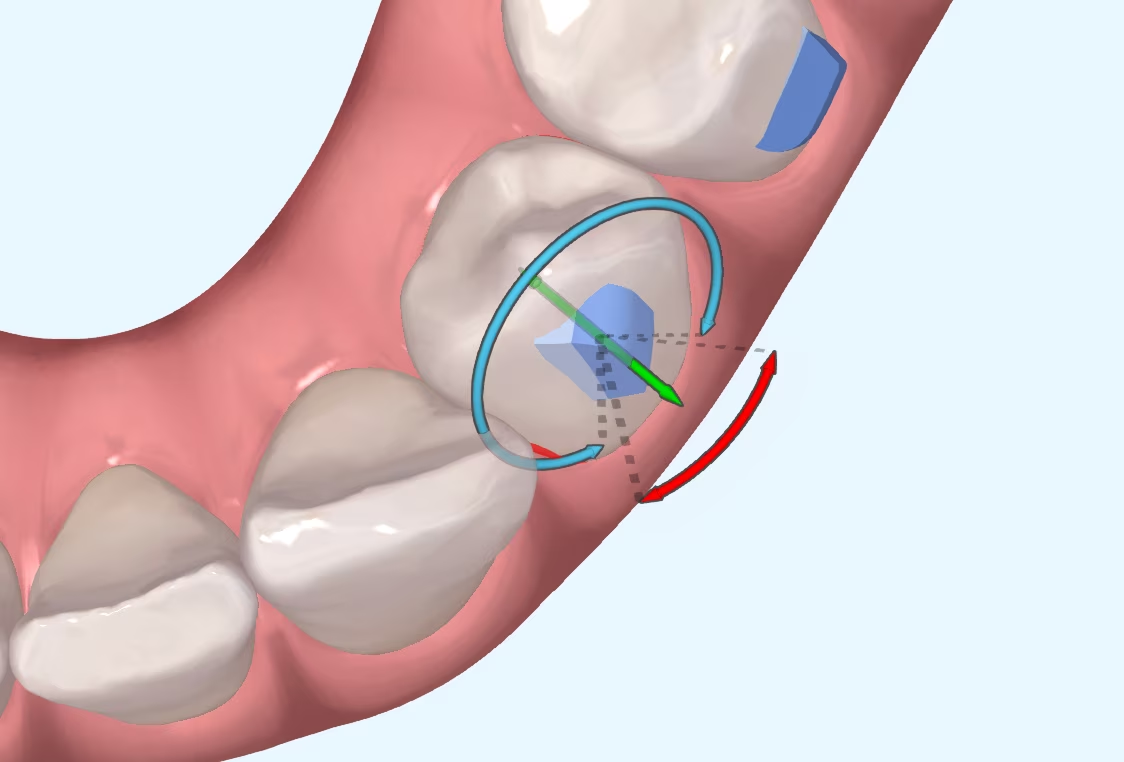
Continuing with the treatment of extractions, in today's blog we will explain other variables beyond the aligners themselves that may influence the predictability of planned movements. We know that mass movement is not possible, that controlling the torque of the anterior teeth during their retrusion is not easy either... but will the same phenomena occur in both arches?
The type of bone present in the maxilla has different characteristics from the mandibular bone, which has thicker cortices and, in general, a
denser bone structure than the upper arch. If the movement of the teeth is conditioned by the surrounding tissues and structures, the upper and lower teeth are more dense.
The lower teeth will not respond equally to the forces we apply to them, whether with braces, aligners or any other orthodontic device.
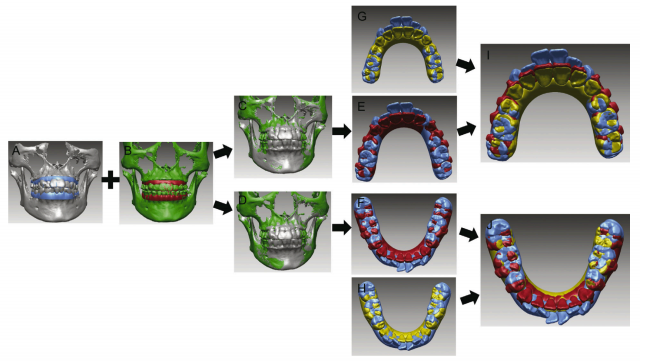
You are at differences between tooth movements in both arches have been studied by Dai et al., who, after performing a series of CBCT overlays on 33
patients undergoing premolar extractions had the following findings:
In the light of the results, we will now summarise their practical application in our extraction treatments:
Dai FF, Xu TM, Shu G. Comparison of achieved and predicted crown movement in adults after 4 first premolar extraction treatment with Invisalign. Am J Orthod Dentofacial Orthop 2021;160:805-13.
Introduction: Initial Considerations If you work with aligners, I'm sure that more than once you've considered changing brands, although most probably

Introduction I suppose many of you are familiar with the myth of Achilles, the Greek hero who was submerged as a child in the River Styx by his mother in order to

What is CBCT? CBCT is a medical imaging technique that uses a special type of computed tomography (CT) scan to obtain three-dimensional images.
Challenges of Overbite In the more than 20 years that we have been working with invisible orthodontics, we have gone from considering some malocclusions "impossible" to daring to

It is not a question to make us feel guilty. It is only a question that invites us to reflect, to think about the impact we can have in