


Integrating sectional arches into clear aligner treatment
Clear aligner treatment does not exclude the use of fixed biomechanics. In certain clinical situations (particularly those involving root control after extraction space closure) a sectional arch offers a level of precision that is difficult to replicate through digital programming alone.
This is not a limitation of aligners. It is a biomechanical decision. And it should be presented to the patient in exactly those terms: not as a failure of the system, but as a deliberate choice within a larger plan.
When sectionals become relevant
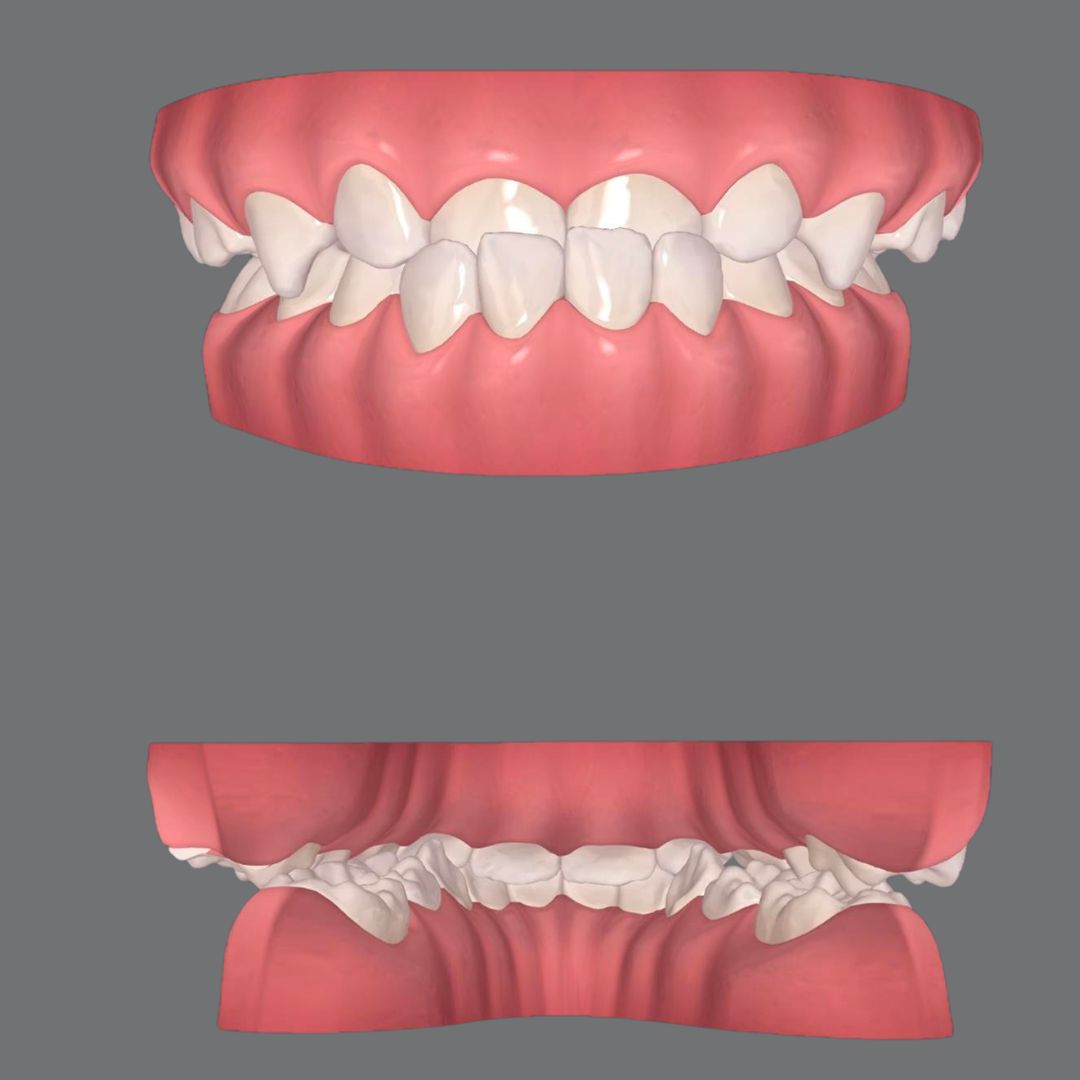
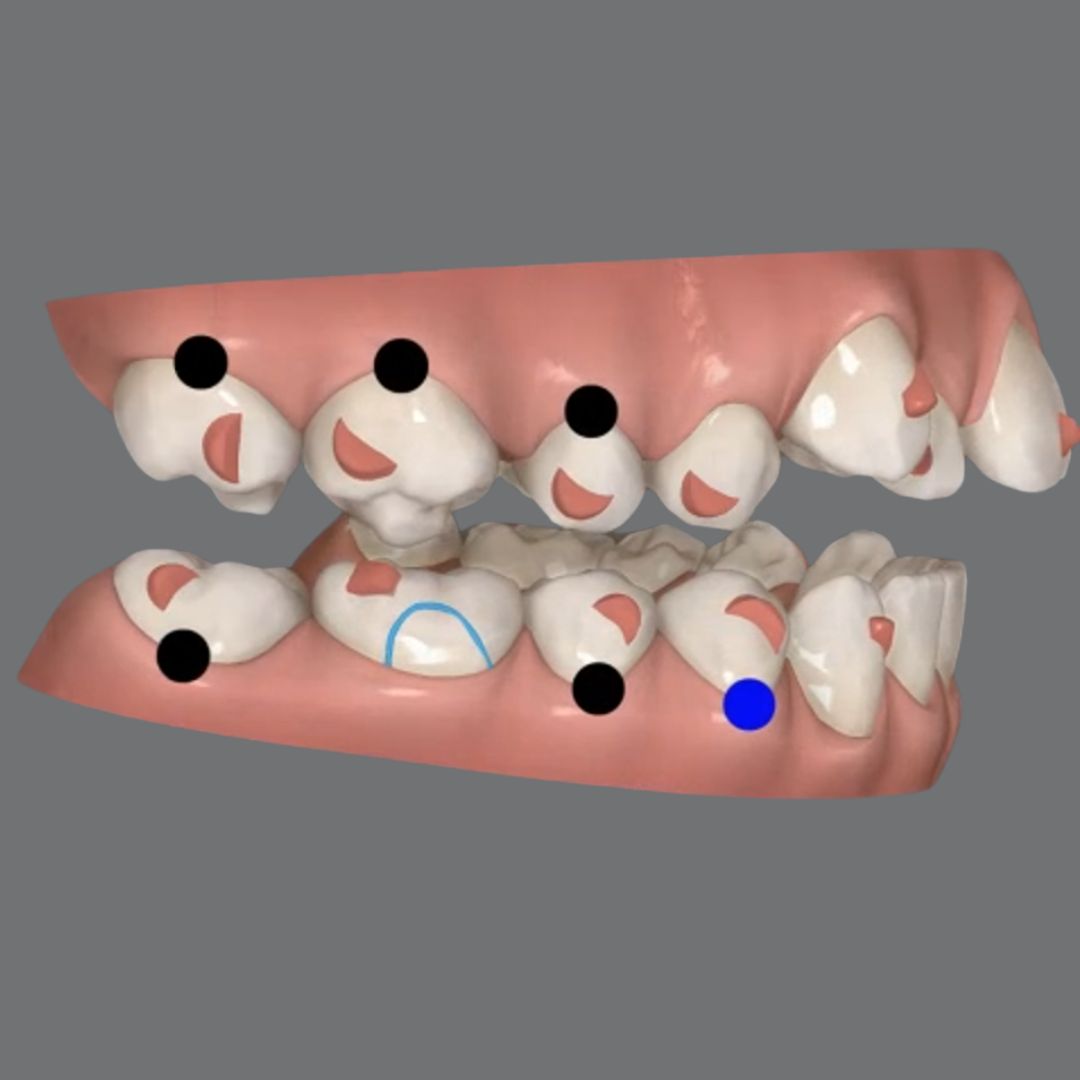
After closing extraction spaces with aligners, root parallelism between canines and premolars frequently requires refinement. Software can program root movements, but the clinical expression of those movements in these specific situations often needs mechanical reinforcement.
A short sectional (typically involving three to four brackets in the relevant zone) allows for a more direct and controlled root moment to be applied. The objective is not to restart treatment with fixed appliances. It is a localized, time-limited intervention with a specific mechanical purpose.
The critical distinction: this intervention should be anticipated from the start of treatment, not improvised at the end.
The trimming design determines the compatibility
Integrating a sectional requires more than simply bonding a bracket. The aligner trimming in that area must be specifically designed to accommodate the bracket and active arch without interfering with the mechanics.
Standard button cutouts are often insufficient in these situations. When the plastic encroaches on the active zone, the system loses efficiency and requires repeated manual adjustments on every tray.
The correct approach is to request a specific cutout from the technician: one that reduces the aligner contour in that zone while maintaining full coverage of the rest of the arch. The aligner continues stabilizing the remaining dentition while the sectional works independently in the target area.
This phase typically spans several consecutive aligners and should be planned as such from the outset.
Biomechanical compatibility: three conditions
A properly designed sectional can coexist with the aligner without interference, provided three conditions are met: the plastic does not invade the active arch zone, the movements programmed digitally are consistent with what will be applied clinically, and anchorage is planned for in advance.
In some cases, elastics complement the sectional mechanics (for example, to reinforce mesial root tip in specific vectors). The goal is to achieve clinically what the digital plan targets, with greater physical control.
Integrating is not mixing: it is planning
The combination of aligners and sectionals should never be reactive. When it works well, it is because it was structured into the treatment from the beginning: a coherent biomechanical plan where each tool has a defined role at a defined moment.
At Smart Aligners Services, this kind of integration is part of what we teach through the SAS Method: knowing when aligners are sufficient, when partial fixed mechanics add precision, and how to design that transition without losing global control.
The difference is not in whether brackets are used. It is in understanding what each phase demands mechanically and planning for it before it becomes necessary.
If you want to learn how to structure combined treatments with this level of control, discover how the SAS Method can help you approach these cases with greater predictability and fewer corrections.
Arch Compression with Aligners: Why Sequence Beats Force
Molar uprighting in a single aligner package
How to avoid interferences in your digitalizations


