
Palatal Expander in Orthodontics, is it worth it?
Will the Palatal Expander be a new revolution? For as long as orthodontics has existed, we have seen different fashions or trends in which priority was given to or
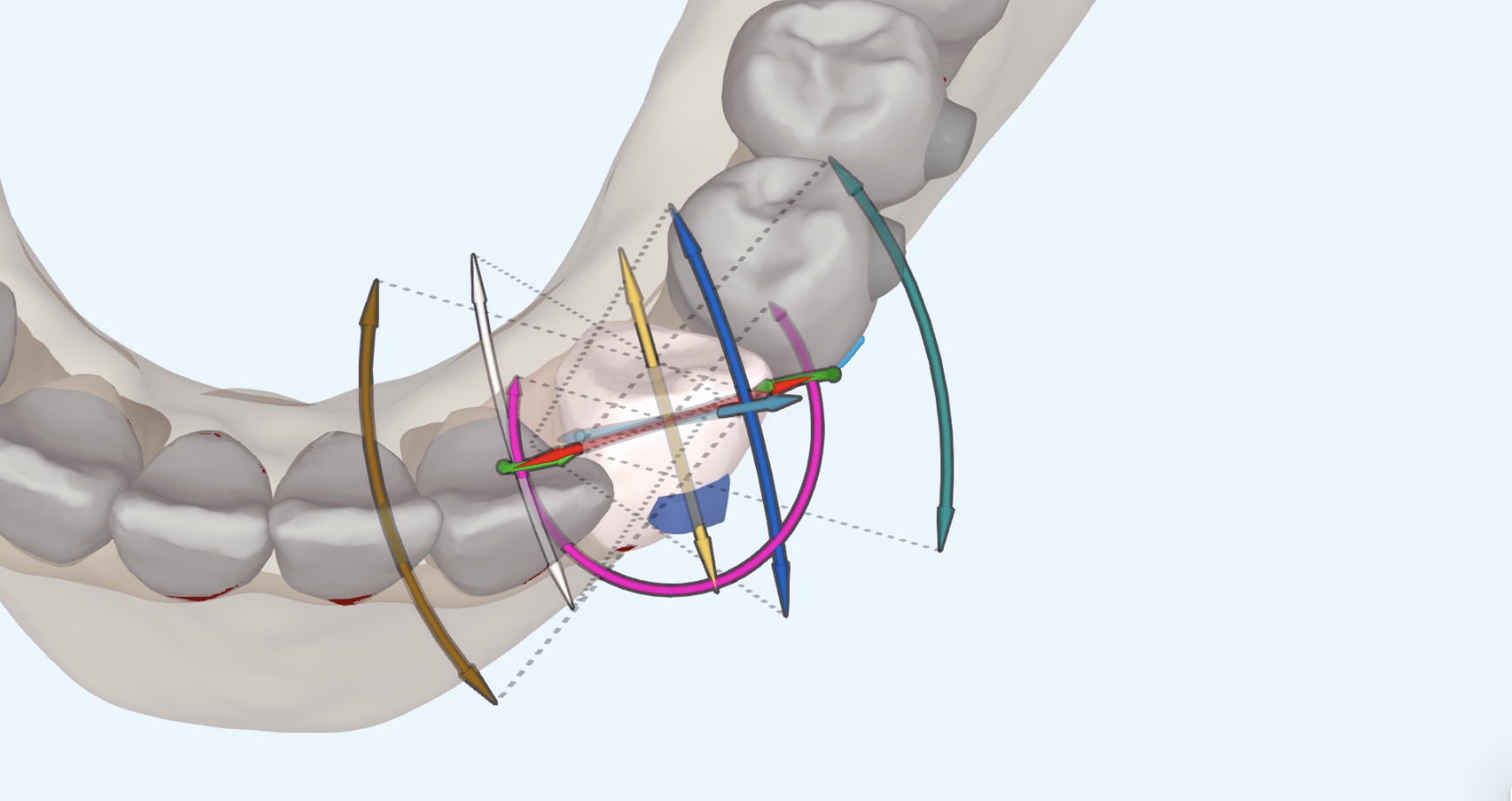
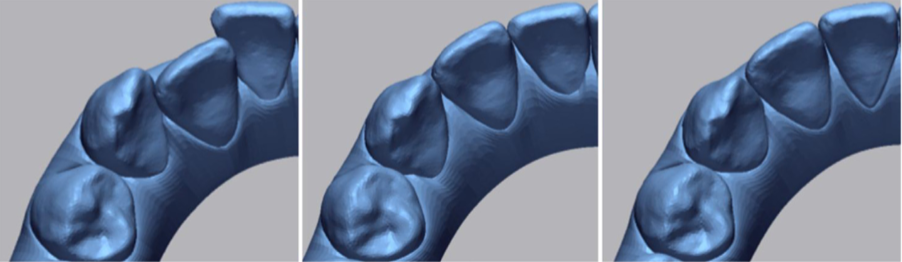
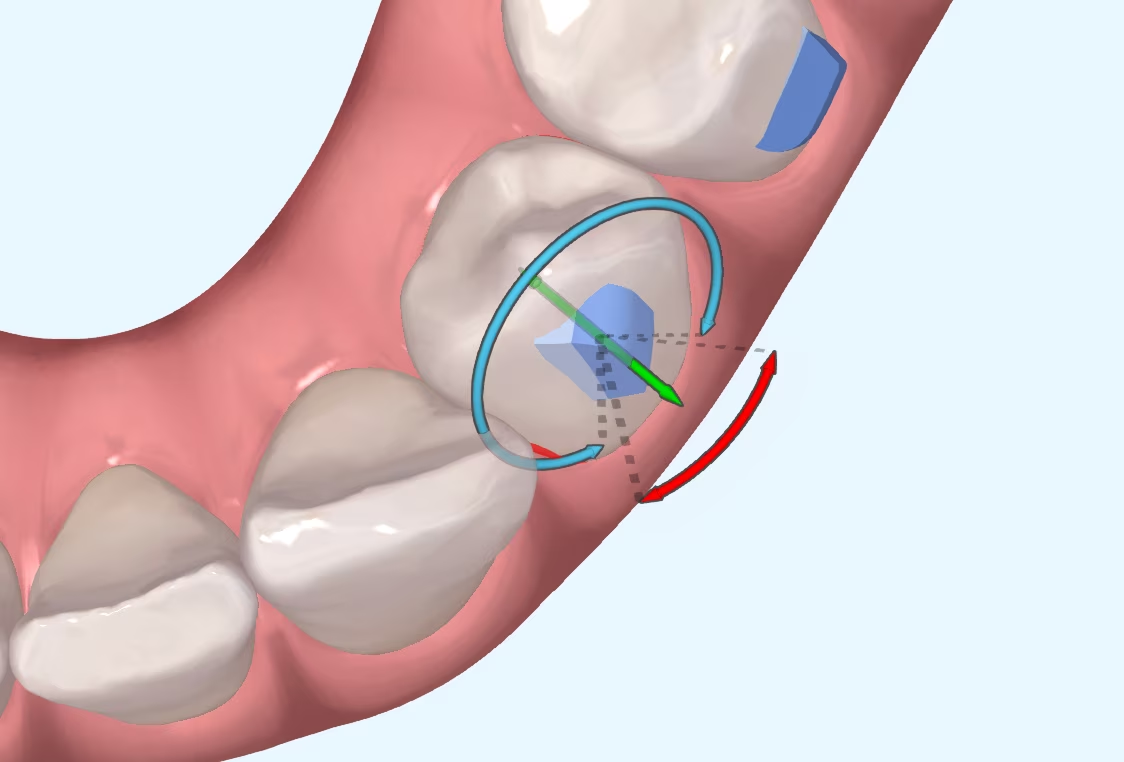
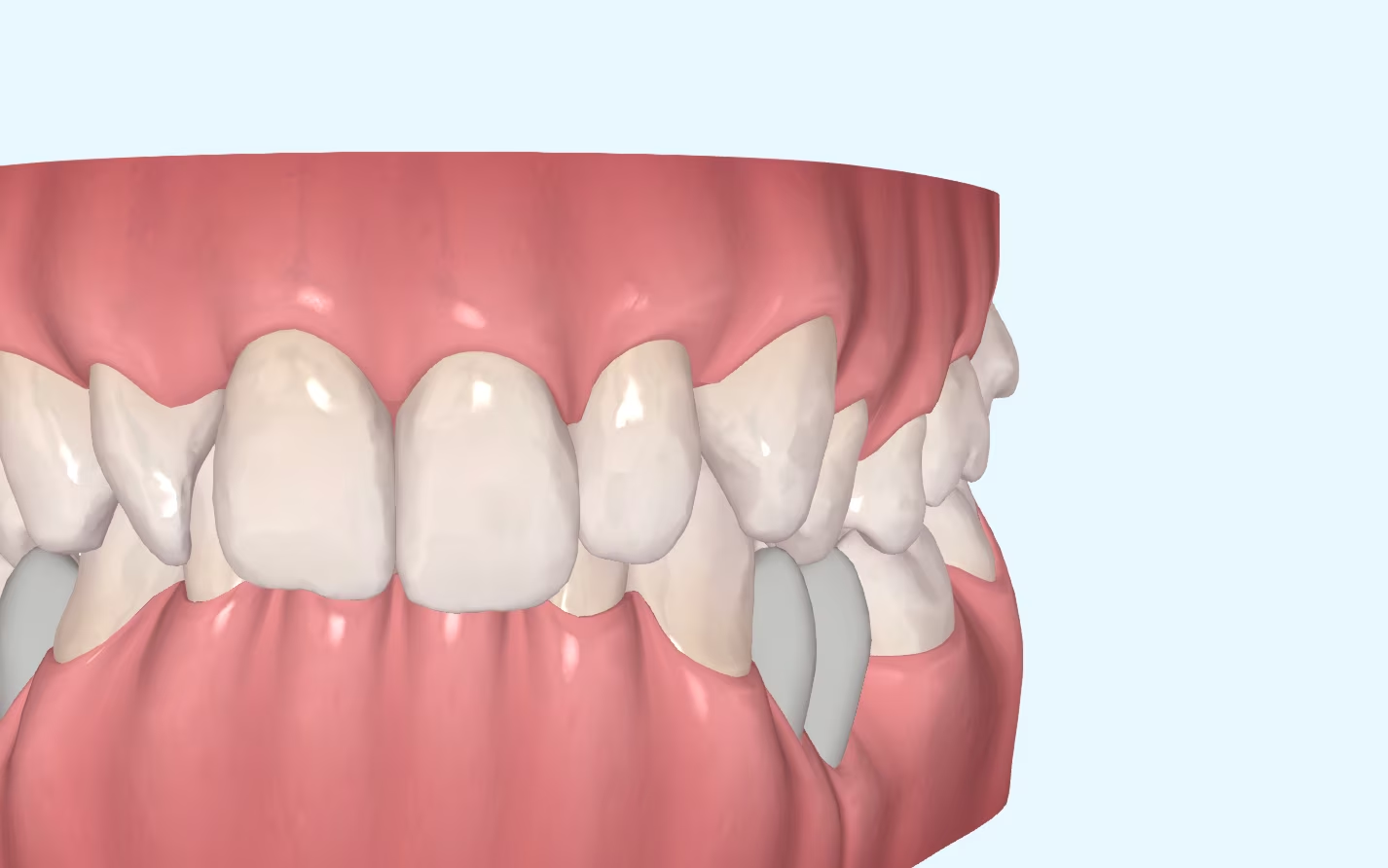
Who hasn't had to scan a patient for a misalignment of a rotated canine? Rotation of round/conical teeth is a movement that can be complex to perform with aligners. The poorly retentive anatomy of the teeth means that the application of forces by the aligners is not as effective as we would like.
To help achieve this movement, the ataches are an essential complement, but they are not the only variable that influences the predictability of the rotational movement of the canines. The type of rotation The type of rotation planned, whether it is a rotation on the axis of the tooth or a rotation with hinged movements, the degrees of rotation of the canine or the protocol for changing aligners can affect the final result and the predictability of the rotation. The differences between the bone of the upper and lower arches should not be forgotten either. The lower density of the upper arch bone compared to the mandibular bone makes lower canine rotations more difficult to achieve.
There are several studies on the capacity of the aligners to rotate these teeth. It is interesting to see how from the early studies by Kravitz et al. in 2008-2009 to more recent studies, such as Stephens et al. predictability of rotation predictability of canines with Invisalign has improved significantly. While in 2008-2009 we had a predictability percentage of around 30% in lower canines, in the study by Stephens et al. they observed an average predictability of 75 %. Despite this, there are also recent studies that have found a lower predictability than that found in this study.
The introduction of the SmartTrack material together with the appearance of optimised attachments for each type of movement depending on the anatomy of each tooth has been an important factor in improving the predictability of rotation. Even so, these improvements have not achieved 100% of predictability, something that is practically impossible to achieve with aligners, regardless of the movement performed.
As expected, given a certain percentage of error, we know that the higher the rotation, the higher the risk of misalignment of the aligner. What do we need to do to improve predictability?
FinallyIt should be noted that these authors have not found significant differences in the predictability of rotation by changing weekly or every 14 days. One possible explanation for this finding may be the fact that in rotations there is no significant root displacement through the bone (as there can be in a case of translation), which is what slows down the movement the most. As there is less bone remodelling, the change every seven days is sufficient to correct the rotation.
One movement, multiple factors to analyse. And, in turn, these factors can be extrapolated to many other movements, which in one way or another will help us to better understand how aligners work. What is clear is that, although they have their limitations, over the years these limitations are becoming more refined and the possibilities for treatment with invisible orthodontics are increasing.
Stephens C. Et al. Clinical expression of programmed mandibular canine rotation using various attachment protocols and 1- vs 2-week wear protocols with Invisalign SmartTrack aligners: A retrospective cohort study. Am J Orthod Dentofacial Orthop 2022;162:e103-e115.
Kravitz ND et al. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop 2009;135:27-35.
Kravitz ND et al. Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign. A prospective clinical study. Angle Orthod 2008; 78:682-7.
Will the Palatal Expander be a new revolution? For as long as orthodontics has existed, we have seen different fashions or trends in which priority was given to or
I suppose many of you are familiar with the myth of Achilles, the Greek hero who was immersed as a child in the River Styx by his mother in order to make him

What is CBCT? CBCT is a medical imaging technique that uses a special type of computed tomography (CT) scan to obtain three-dimensional images.
Challenges of Overbite In the more than 20 years that we have been working with invisible orthodontics, we have gone from considering some malocclusions "impossible" to daring to

It is not a question to make us feel guilty. It is only a question that invites us to reflect, to think about the impact we can have in

Maxillary compression is a relatively frequent problem seen in our daily practice. This osseodental discrepancy presented by the patient can be treated in the following ways