
Palatal Expander in Orthodontics, is it worth it?
Will the Palatal Expander be a new revolution? For as long as orthodontics has existed, we have seen different fashions or trends in which priority was given to or

Extraction cases with aligners are considered some of the most complex cases to treat with aligners. due to the properties of the plastic. When treating extractions with brackets, we have the possibility to choose the stiffness and thickness of the archwire to achieve greater control of the mass movement of the teeth during space closure. However, in treatments with aligners we do not have this possibility.
To make up for these shortcomings, aligner companies have devised different systems. For example, InvisalignThe new system, despite using the same type of plastic, introduces additional forces to improve the root control of the teeth. Others, such as Orthocaps o Angel AlignThe aligners combine aligners of different stiffness throughout the treatment to achieve better control of movement. The latter work in a very interesting way: each stage consists of two aligners, one more flexible and the other more rigid. The latter serves to "consolidate" the movement, achieving a priori a more predictable movement.
If we leave aside the type of plastic we are going to use and focus on the mechanics of the alignersIn order to be able to plan virtually, it must be understood that virtual planning is a way to
The Clincheck is a way for orthodontists to create a system of forces that we will later apply to our patients' teeth when the aligners are fitted. The ClinCheck does not always reflect the final position we want to achieve. This discrepancy between the final situation on the ClinCheck and the actual situation of the patient's teeth increases as the difficulty of the case increases.
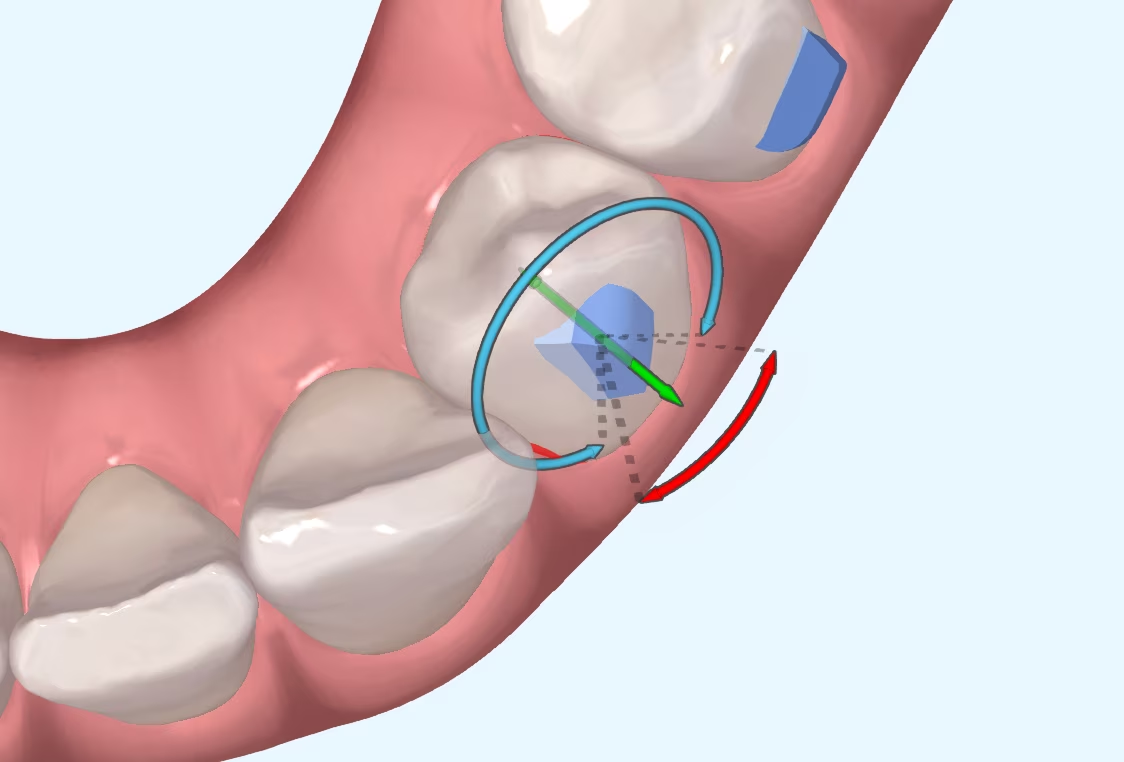
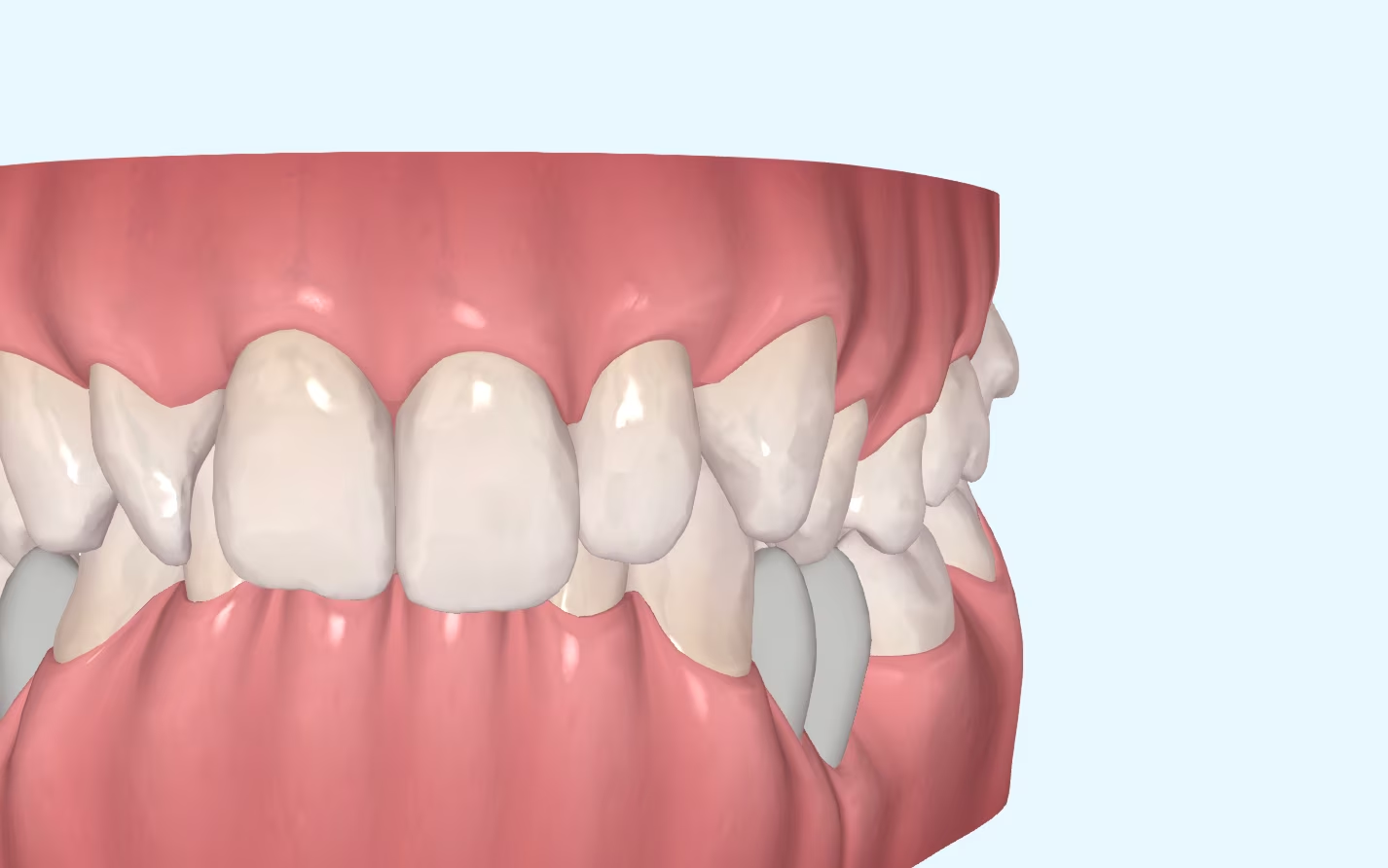
When we close an extraction space, the teeth tend to tilt towards the extraction space. If, for example, we have extracted a first premolar, the canine will tilt distally into the space and the molars and second premolar will tilt mesially into the space. Even if we have planned a mass movement in the ClinCheck to close the gap, it is difficult to do it this way.
As is often the case, it is difficult to determine a specific number of degrees. What is clear is that, the greater the translational movement, the greater must be the
overcorrection. You can see an example of the study carried out by Feng et al. in which they show the recommended degrees of overcorrection for anchor cases
maximum in which space closure is achieved mainly by anterior retrusion.
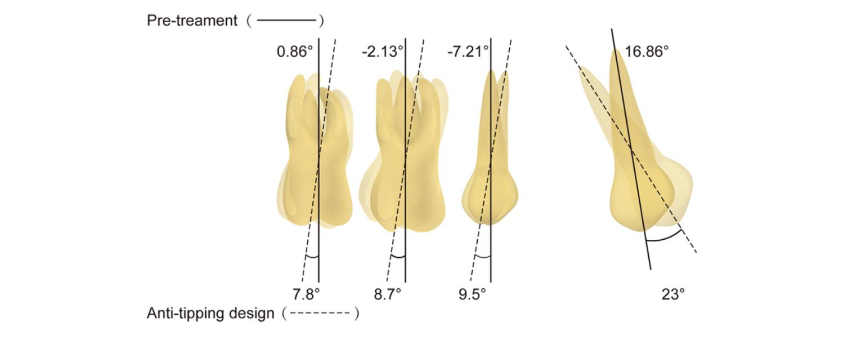
If we look at these values, we can see that the canine, as it has a greater retraction movement, will need more degrees of overcorrection (coronodistal tip). The molars and the second premolar, which act as anchorage teeth, have about 8º-9° of coronodistal tip, which increases the posterior anchorage and prevents their mesialisation.
We must not forget that, even if we make these overcorrections, mass movement is very difficult to achieve, and there are many more factors that influence it.
The use of a dental crown is a very important factor in the achievement of these goals (the size of the clinical crowns, the inclination of the teeth, the presence or absence of crowding...) so we will have to be prepared to use
auxiliary tools with which to finish straightening the teeth and close the extraction space correctly if the aligners fail to do so.
Feng X et al. Comparison between the designed and achieved mesiodistal angulation of maxillary canines and posterior teeth and influencing factors: First premolar extraction treatment with clear aligners. Am J Orthod Dentofacial Orthop 2022;162:e63-e70.
Will the Palatal Expander be a new revolution? For as long as orthodontics has existed, we have seen different fashions or trends in which priority was given to or
I suppose many of you are familiar with the myth of Achilles, the Greek hero who was immersed as a child in the River Styx by his mother in order to make him

What is CBCT? CBCT is a medical imaging technique that uses a special type of computed tomography (CT) scan to obtain three-dimensional images.
Challenges of Overbite In the more than 20 years that we have been working with invisible orthodontics, we have gone from considering some malocclusions "impossible" to daring to

It is not a question to make us feel guilty. It is only a question that invites us to reflect, to think about the impact we can have in

Maxillary compression is a relatively frequent problem seen in our daily practice. This osseodental discrepancy presented by the patient can be treated in the following ways