One of the great debates in orthodontics that has been going on almost since its inception is the need or not to make extractions. Looking back, it is interesting to see how this issue has fluctuated over time, with the creation of orthodontic trends or 'currents'. who defend the need for extractions or, on the contrary, the possibility of treating practically all patients without extractions. The concept of treatment without extractions has even been used as an advertising gimmick to offer patients an a priori more attractive treatment (nobody likes having teeth removed) but without considering the long-term consequences. Just as each person has different feet and there are different shoe sizes for each one of them, orthodontic treatment should also be adapted to each individual's needs. plan tailored to the individual patient's malocclusion and biological limits.
Whether or not to extract does not depend on the appliance we fit the patient with. Whether with brackets or aligners, the need for extraction will be determined after a exhaustive diagnosis of the case. However, depending on the technique we use, we may opt for one extraction or another depending on the biomechanics we want to apply. For example, if we have a complete Class II case, it is possible that if we treat the case with aligners, we will opt for extracting wisdom teeth and, if we have a complete Class II case, it is possible that if we treat the case with aligners, we will opt for extracting wisdom teeth.
we treat it with brackets, we decide to extract premolars.
Why? Because we know that closing premolar spaces with aligners is biomechanically more complex to achieve than upper distalisation, whereas with brackets, by having better control of root movement, we can close these spaces in a more efficient and predictable way.
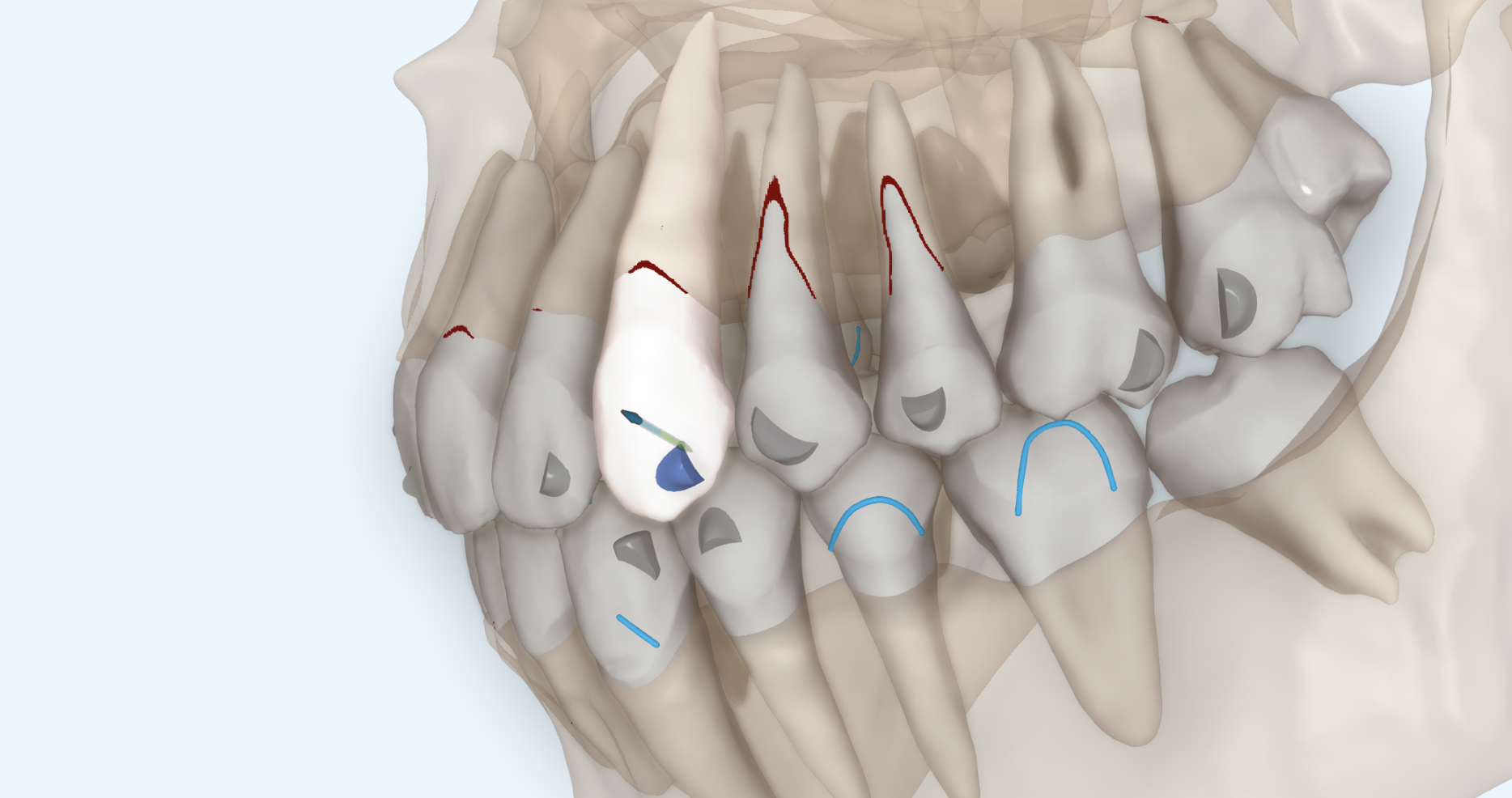
Fenestrations and dehiscences
Fenestrations and dehiscences of the alveolar bone are defects that are naturally present in many people; it is not necessary to undergo orthodontic treatment for them to appear. It is also true that, after orthodontic treatment, these defects increase.
If we review the articles on this subject, it is interesting to see how the increase in recessions and dehiscences after treatment with brackets ranged from 10% to 20% while, in cases treated with aligners, they only increased by 4%. These are few articles, with different methodologies, so these numbers should be taken with a pinch of salt. But they give us a clue about the greater control that brings us the digital planning with aligners versus conventional treatment, where we cannot always control the pro-inclination and expansion of the teeth. Brackets may be biomechanically superior to aligners in certain movements, but aligners are clearly superior in terms of control.
We already know that orthodontic treatment increases the risk of creating fenestrations/dehiscences or increasing them if they are present from the start. But... is this risk the same in all cases?
Let's look at the variables involved:
- Age: The older the patient is, the slower the bone metabolism and the worse the patient's response to tooth movement, which translates into a higher risk of fenestrations/dehiscence.
- Bone area: As a general rule, most bone defects are located in the vestibular cortex, with a greater presence in the maxilla than in the mandible.
- Race: African-American patients have a higher percentage of fenestrations/dehiscences compared to Caucasians, possibly due to greater proinclination of the anterior teeth.
- Angle ANB: There is a directly proportional relationship between the ANB angle and the presence of fenestrations/dehiscences.
- Expansion: The greater the planned expansion, especially if we start from a posterior torque close to 0º, the greater the risk of creating or increasing bone defects.
Knowing these variables, we will be able to analyse the case more precisely and decide whether or not extractions are necessary. The use of CBCT is also a great help to see the consequences of the movements we plan, but it cannot replace orthodontic knowledge. This tool has a certain margin of error and is not able to simulate bone remodelling, so it is advisable to take these variables into account when treating our patients.
Allahham DO et al. Association between nonextraction clear aligner therapy and alveolar bone dehiscences and fenestrations in adults with mild-to-moderate crowding. Am J Orthod Dentofacial Orthop 2023;163:22-36.