
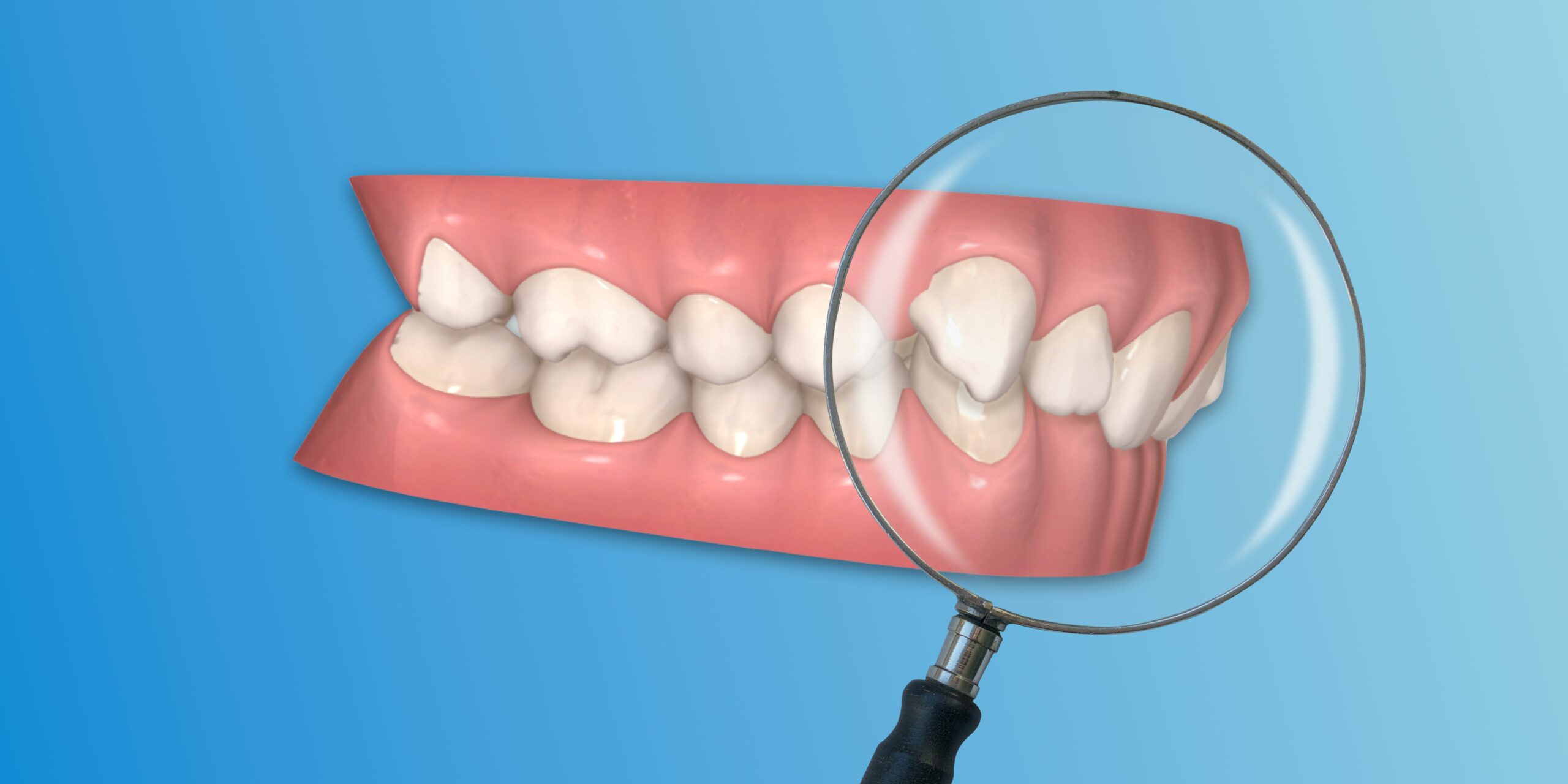
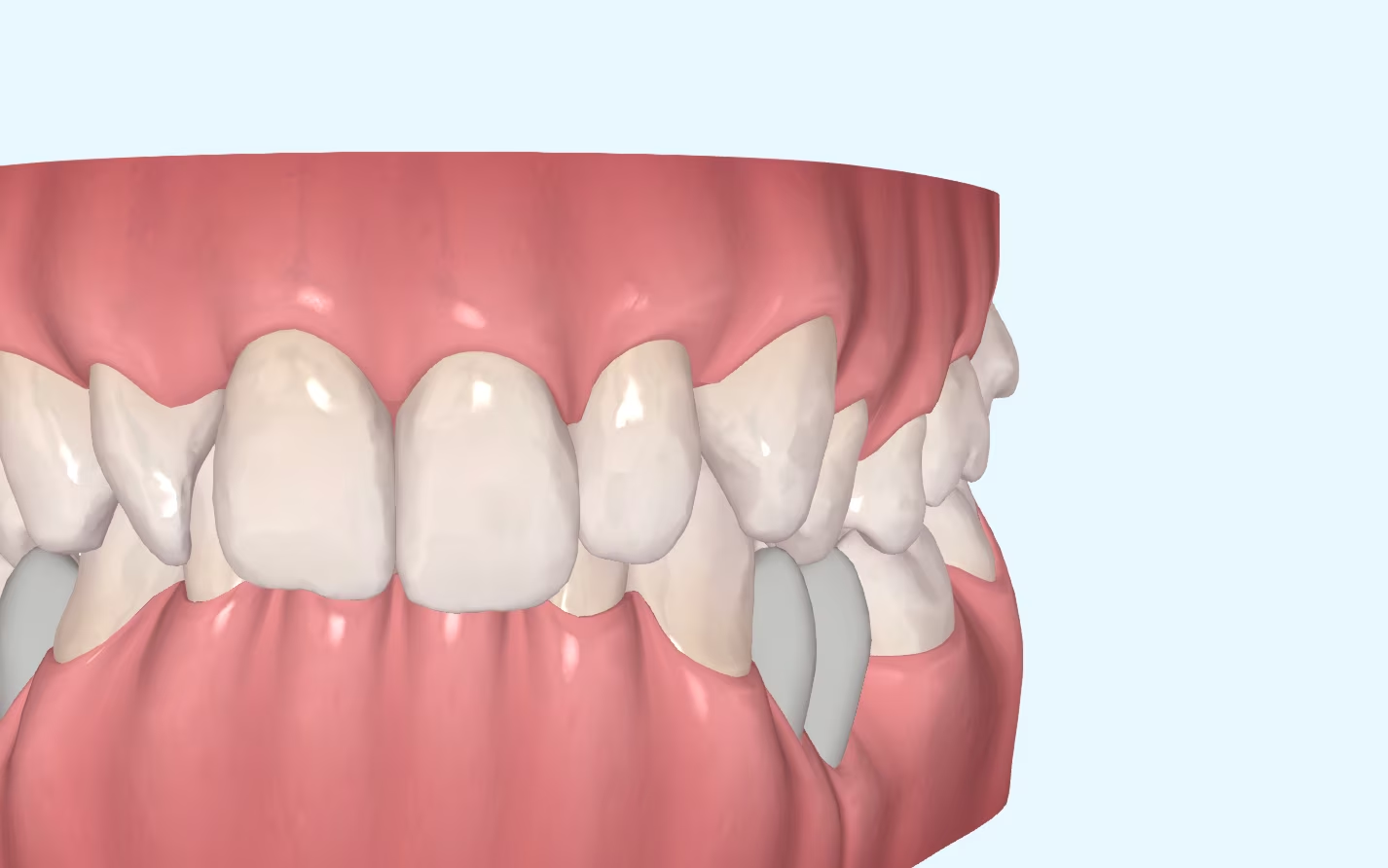
Class II malocclusion is one of the most common malocclusions among orthodontic patients. Within Class II, there are two sub-types, division 1 and division 2. dental and facial characteristics that will need to be taken into account when designing our treatment plan. For example, among patients with Class II division 2 it is common to observe that they are patients with a concave profile, recessed lips, a reduced lower third and a prominent chin. Intraorally, we will find mouths with a lot of compression, retro-inclined incisors and increased overbite.
Class II division 2 can be treated with aligners or with brackets, achieving similar results. However, the biomechanics of the two are different. Studies show that the effectiveness of both devices in correcting this malocclusion is similar.. In my opinion, or at least in my hands, torque correction is easier (or faster) to achieve with fixed orthodontics compared to aligners. When a patient has incisors with very negative torque and a complete overbite, I find it more difficult to treat this type of problem with aligners alone than, for example, with brackets and a pair of archwires.
Australians with tip-back.
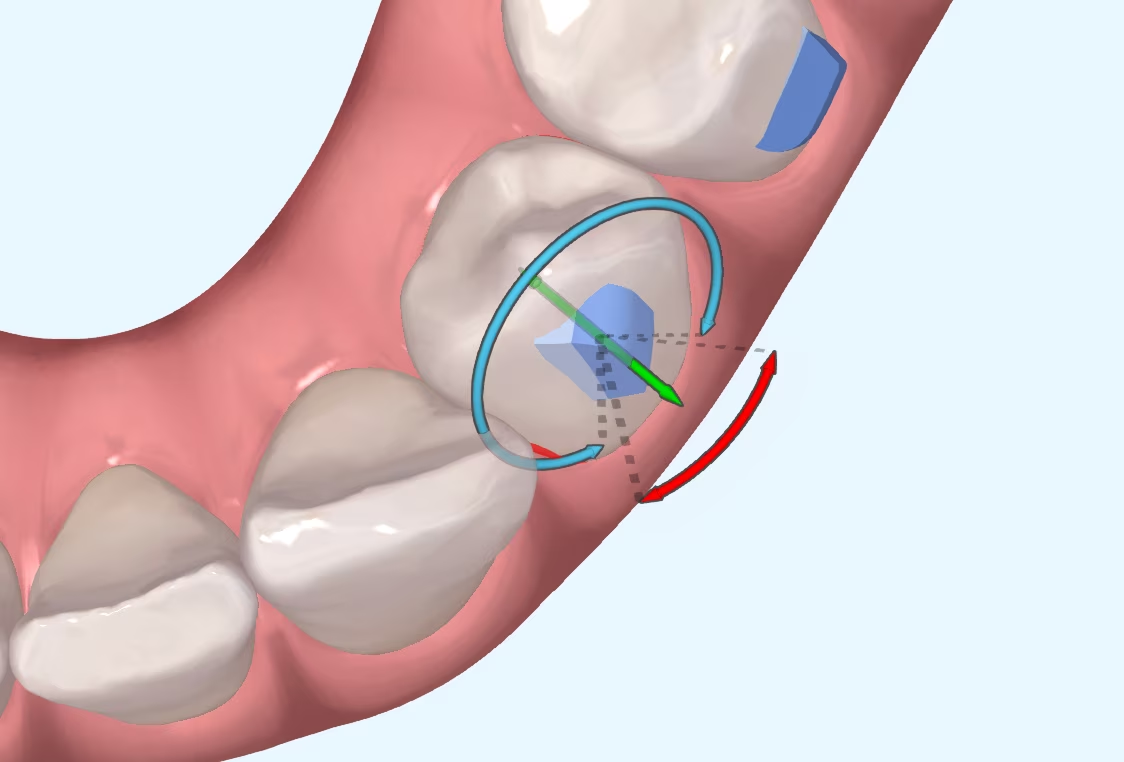
Although the mechanics of fixed orthodontics have an older origin than the mechanics of aligners, they are still more effective for certain movements. Proof of this can be seen in those cases of aligners where we need to place sectional arches to improve the tip or root inclination of the teeth or when we place buttons and chains to unrotate a tooth that has fallen behind. The ease with which we manage to change the torque and improve the overbite with fixed orthodontics is not possible with aligners, as they are removable. For this reason, when we have very complex cases of class II division 2, we will sometimes need auxiliary tools to the aligners, such as micro-screws, which will help us to achieve the desired torque.
However, although braces may be more effective than aligners in correcting this type of malocclusion, this does not mean that they are the best option in all cases.
One of the unwanted effects caused by almost all orthodontic treatments is the root resorption associated with tooth movement. The exact reason for this problem is difficult to determine, as there are numerous risk factors that can cause this root resorption: from gender, age, race, type of movement, the amount of force we apply, the length of time of orthodontic treatment... and there is also another variable that we must not forget: the type of appliance we use. And in this aspect, aligners outperform braces (by a small margin).
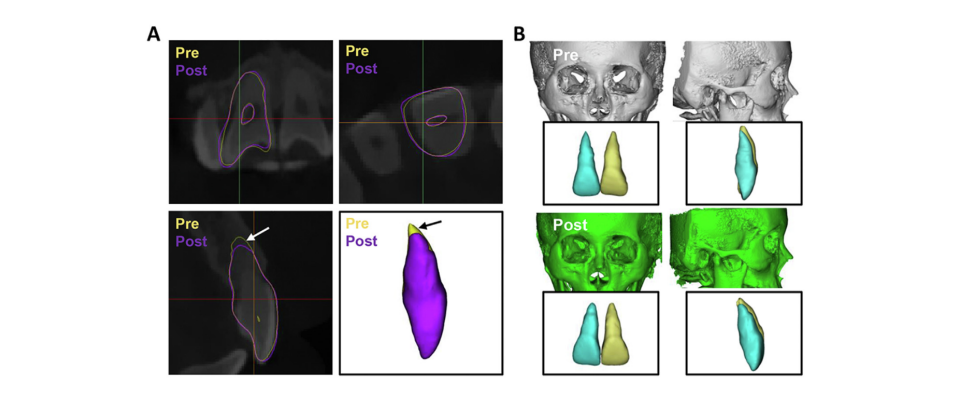
A recent study has shown that the root resorption caused in Class II 2 treatment with aligners is less What are the reasons for this? We can identify two main reasons:
Therefore, in cases of Class II division 2, the following dilemma arises: what is more important: correcting the malocclusion with brackets and playing it safe, or treating the patient with aligners, knowing that it may be a more complex treatment but that it can reduce the amount of root resorption? As always, there is no right answer. It will depend on the case.
Chen H et al. Changes of maxillary central incisor and alveolar bone in Class II Division 2 nonextraction treatment with a fixed appliance or clear aligner: A pilot cone-beam computed tomography study. Am J Orthod Dentofacial Orthop 2022.
I suppose many of you are familiar with the myth of Achilles, the Greek hero who was immersed as a child in the River Styx by his mother in order to make him

What is CBCT? CBCT is a medical imaging technique that uses a special type of computed tomography (CT) scan to obtain three-dimensional images.
Challenges of Overbite In the more than 20 years that we have been working with invisible orthodontics, we have gone from considering some malocclusions "impossible" to daring to

It is not a question to make us feel guilty. It is only a question that invites us to reflect, to think about the impact we can have in

Introduction: Understanding Maxillary Compression Maxillary compression is a relatively common problem seen in our daily practice. This osseodental discrepancy that presents the