I remember when I was immersed in the world of aligners. In those first trainings, we were shown the strengths and weaknesses of invisible orthodontics. For example, a case with an open bite could be easier to resolve with aligners than with braces, thanks to the intrusion produced by the forces exerted by the patient on the aligners in the posterior area. However, these forces, which are so useful for closing bites, worked against us in cases of increased overbite.
It is not appropriate to generalise, but a large part of the patients with an enlarged overbite have high muscle tone and clench their teeth. In these patients it is easy to see how unwanted intrusion occurs. This effect is difficult to avoid, even with bite ramps, as the ramps that appear in aligners are not as effective as the ramps or stops that we place with fixed orthodontics for two reasons:
- The ramps, being part of the aligner, are removable. As they are not fixed to the teeth, they have no effect when the patient removes the aligners.
- They tend to have less contact than ramps fitted with brackets, which can be completely customised to each case. They can even be useless in cases with a lot of protrusion, as they have a limited length and in these situations they will not contact the lower incisors.
To make up for these shortcomings, we have other strategies, such as manually making the ramps and scanning the patient so that they appear manufactured in the aligners. We will leave this subject for another article.
In the first published studies on the effectiveness of aligners and brackets in correcting overbite, they found that brackets were far superior to aligners (approximately 50% more effective). Years later the performance of aligners in deep bite cases has been re-analysed and surprisingly they have found similar efficacy to brackets. It is true that there are always differences in the methodology of the studies, but it is interesting to see how, since the appearance of G5, the results have improved. The advent of bite ramps, optimised attachments and Smart Forces designed specifically for this malocclusion, together with the increased understanding of aligner biomechanics, have made it possible to treat these patients and achieve acceptable results.
In the study by Fujiyama et al. we see how the correction of overbite with brackets produces greater posterior extrusion than treatment with aligners and that, when correcting an overbite with aligners, it will be resolved mainly by anterior intrusion (1 mm of intrusion of upper incisors and 2 mm of intrusion in lower incisors). Depending on the vertical dimension of the patient, the extrusion produced with fixed orthodontic treatment may or may not be favourable, as it will increase the vertical dimension and, in adult patients, this may cause mandibular posterorsion. With aligners we will have a better
control of the vertical dimension, but we will be very limited if we want to achieve correction of the overbite with posterior extrusion.
However, there are a number of other independent factors to the aligner system, which are of vital importance to understand the degree of difficulty of the overbite to be treated:
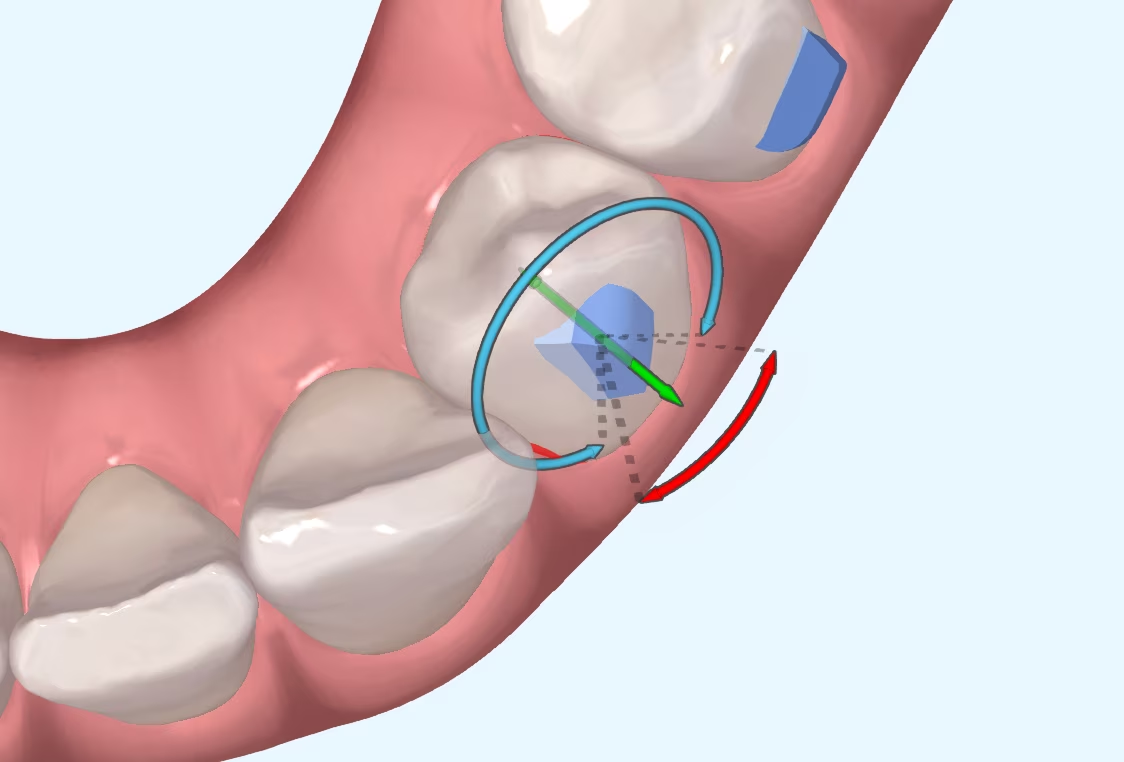
- Pure intrusion vs. relative intrusionPure intrusion is a less predictable movement than relative intrusion produced by proinclination of the incisors. Depending on the anterior torque of the patient, the correction of the overbite will be more or less predictable. In a case where we have negative torque, we will have more proinclination and, therefore, it will be easier to correct the overbite.
- Amount of crowdingThe greater the amount of crowding, the easier it will also be to resolve the overbite, as the correction of crowding is always associated with a certain amount of proinclination, even when stripping. For this reason, when we are faced with a case with all the anterior teeth aligned, we should be aware that it will be more difficult to achieve intrusion of the anterior teeth.
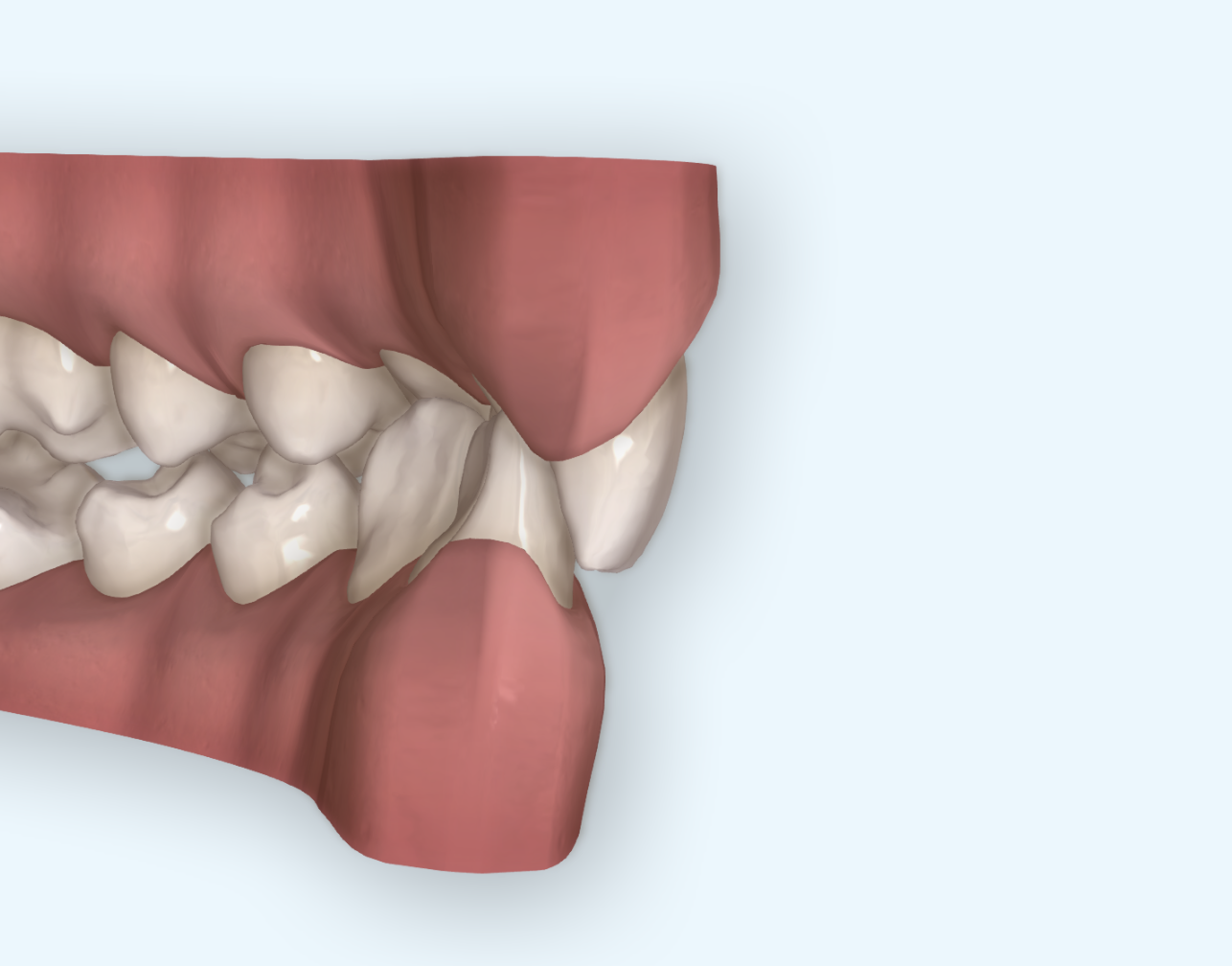
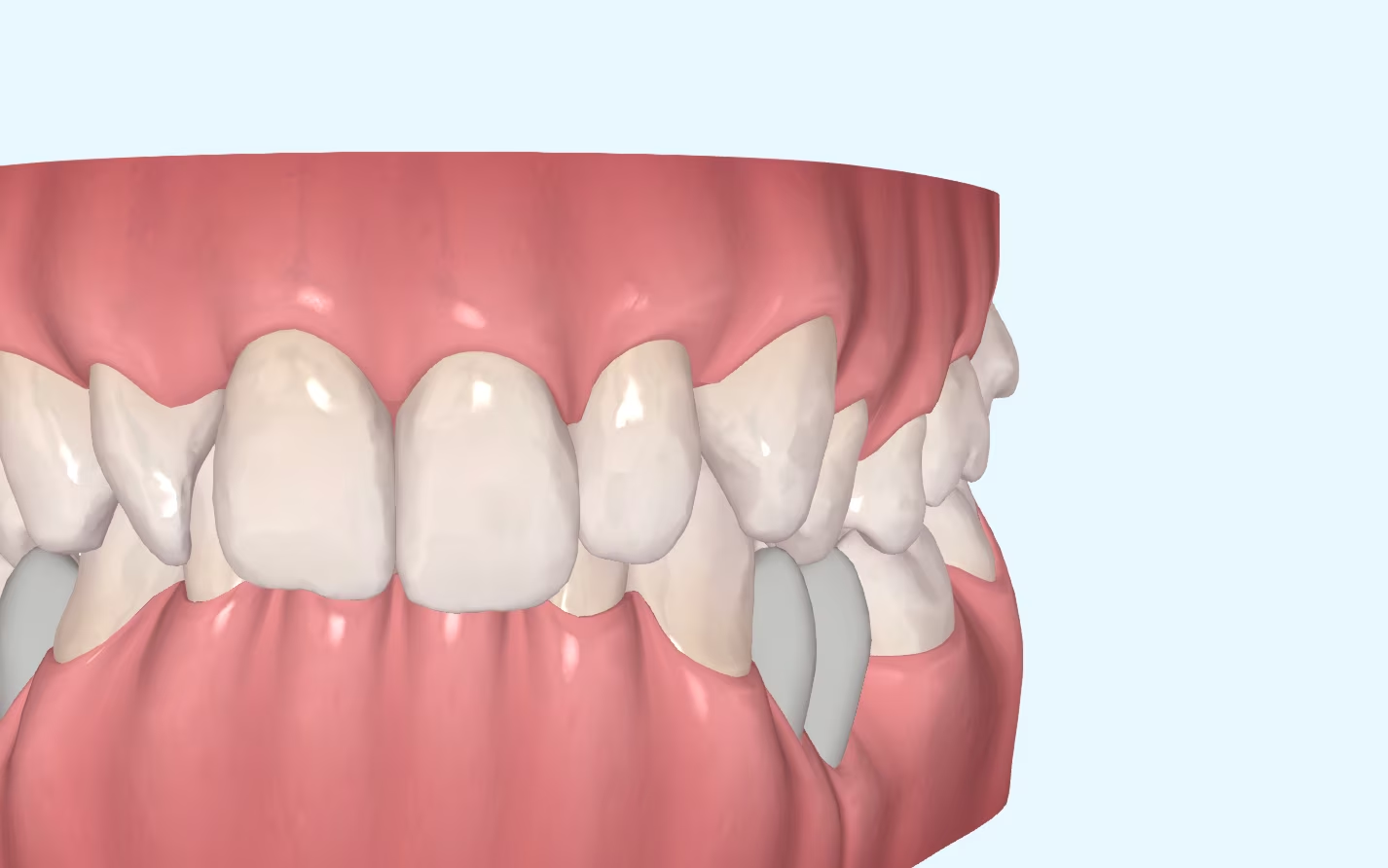
- Number of teeth to be insertedWhen measuring the overbite, we look at the number of millimetres that the upper incisors cover the lower incisors, but not all overbites are the same. An overbite of 100% on lower incisors with relatively well positioned canines is not the same as an overbite where both canines and incisors are equally extruded. The intrusion of the incisors will be more predictable than the intrusion of the six anterior teeth (canines and incisors).
At the same overbite value, each case will present a different complexity, which is why we cannot be guided solely by the numerical diagnosis. It is advisable to analyse the patient's clinical conditions in detail and determine the viability of the case with invisible orthodontics on the basis of these conditions. Once the complexity of the malocclusion has been discerned, we can decide whether auxiliary tools, such as micro-screws, are necessary or whether aligners are sufficient to resolve the overbite.
Krieger E et al. Invisalign treatment in the anterior region: were the predicted tooth movements achieved? J Orofac Orthop 2012;73:365-76.
Fujiyama K et al. Comparison of clinical outcomes between Invisalign and conventional fixed appliance therapies in adult patients with severe deep overbite treated with nonextraction. Am J Orthod Dentofacial Orthop 2022;161:542-7.